The Impact of COVID-19 on College Students – Understanding the implications of the COVID-19 pandemic in a global society is critical as it founds preparation for potential health crises. The pandemic resulted in a critical death rate internationally, which has had detrimental effects on relatives’ psychological well-being (Coughenour et al., 2020).
Second, with the infection rates requiring expensive treatment facilities and resources, destabilization of the global public health sector was apparent. Furthermore, the pandemic altered nations’ economies by distorting employment, ultimately inducing people to low living standards, resulting in trauma and depression (World Health Organization, 2021). Such impacts are practical and evident in society at large, including college students.
Researchers have documented the social, economic, and psychological implications of COVID-19 in society. According to Chriscaden (2020), the pandemic increased poverty rates, raising the number of undernourished people by 132 million individuals.
Such statistics imply that the population suffering poverty-induced mental instability significantly increased with the pandemic. With over 1.8 million deaths globally by the end of 2020 for only countries that can quantify the cases effectively, the social and psychological impacts of the COVID-19 pandemic are inarguable (World Health Organization, 2021).
Overall, whether social, economic, or mental implications of the pandemic, the apparent harmful implications in the global community, at all ages, races, ethnic groups, and other social classes.
Specifically, college students should understand how the pandemic affected their social, economic, and psychological welfare to relate effectively and understand how their situations matched the practical health crisis implications. Such research offers the fundamental data and information to spur awareness and attention on the need to focus on college students when health crises occur.
According to World Health Organization (2021), the impacts of the pandemic on the global education system have had a deleterious implication on learners. Therefore, as nations focus on restoring the vulnerable population’s well-being, college students should not be excluded.
College students significantly suffered the pinche of the COVID-19 pandemic considering the social, economic, and political elements surrounding the health crisis. When the World Health Organization (WHO) pronounced the pandemic as a global health crisis, national governments had to take stringent measures to curb the infection spread, including barring physical and interactive classes in colleges.
Such a move distorted the higher learning bussing culture and proximity, inducing learners to critical psychological challenges. College students who were on internships lost their livelihoods, predisposing them to hard financial situations.
The death of relatives and friends due to the critical nature of the COVID-19 infections also pushed college students to hard life situations characterized by psychological and mental instability.
Therefore, although society might not focus on the college students significantly, they form a key group of individuals who suffered the pinches of the COVID-19 pandemic.
Literature Review
Researchers have exploratively studied the impacts of the COVID-19 pandemic on college students. With the practical effects of the pandemic on human health, including the substantial death rate, and the stay-at-home order in the United States (US), scholars have concluded significant implications in different research journals. Coughenour et al. (2020) and Lee et al. (2021) are among the key researchers exploring the pandemic’s implications on US college students.
Coughenour et al. (2020) explore the correlation between the stay-at-home order, learners’ involvement in physical activity at home, and psychological welfare. Their findings highlight that the pandemic had substantive negative effects on college students’ physical activities and psychological well-being.
Such inference implies that the indoor stay at home reduced the students’ involvement in physical exercises, which integrated with such other factors as the deaths of relatives and friends to contribute to stress and depression.
Also, the journal article concludes that non-American college students suffered more than American learners during the pandemic. Such inference implies that parents, guardians, the government, and the education fraternity should significantly focus on the students of color when health crises occur.
Impact of COVID-19 and Psychological implications
Lee et al. (2021) explores the social and psychological implications of the pandemic on US college students. The authors conclude that the pandemic significantly distorted the college students’ psychological welfare by minimizing physical interactions.
With the barn of physical classes and the indoor lifestyle, students had unreliable social interactions that augmented stress and depression. Ideally, the pandemic distorted the learners’ social life, inducing them to psychological instability. Also, the journal article highlights no significant social differences in the impacts of the COVID-19 pandemic. Such inferences oppose the common expectation that such groups like the LGBTQ+ and non-white students suffered many more challenges than the American students.
While the two research articles focus on different elements regarding the impacts of the pandemic on US college students, social versus psychological, they both posit critical alteration of mental welfare. For Coughenour et al. (2020), failure to engage substantially in physical activities during the pandemic and other social and economic conditions alter the students’ mental welfare.
The Impact of COVID-19 on College Students
Similarly, Lee et al. (2021) denote that the socioeconomic implications of the pandemic played a critical role in triggering depression and stress among college students. Both articles present practical arguments because inadequate engagement in physical activity, unreliable social interactions, loss of family members, and financial strains, to mention a few factors, would disrupt mental well-being.
Therefore, both articles reinforce damaging factual implications of COVID-pandemic on college students, recommending future comprehensive research to explore the subjects. However, the articles differ in defining the social variation of the pandemic implications on various social groups, including the blacks and the LGBTQ+ community.
Although Coughenour et al. (2020) infer significant differences of implications relating to sexual orientation, Lee et al. (2021) findings indicate no significant differences in any social group. Although the opposing inferences from both research works might be confusing, the differences in focus might have caused the diverse conclusions.
Notably, the often-societal discriminated groups, including the LGBTQ+ community and the blacks, might have perceived the indoor stay as an opportunity to evade stigmatization, hence evading outdoor physical engagements. Contrary, Lee et al. (2021) emphasize that the presence of strong organizations and groups supporting the minority groups provided reliable support during the pandemic, minimizing psychological breakdown among member college students. Therefore, the evident differences between the two articles are due to focus, which is normal in research studies.
Conclusion
In a nutshell, the COVID-19 pandemic is a fundamental health crisis, and its implications affect every member of society, including college students. Coughenour et al. (2020) and Lee et al. (2021) prove that the epidemic had deleterious impacts on college students’ welfare.
With alteration on learners’ social, economic, and psychological welfare, destabilization of individuals’ welfare was apparent. Such a fact requires the education sector and the global public health system to prepare adequately for future health crises and consider college students’ mental well-being as a key aspect. Researchers are also stakeholders as they will help offer objective findings, which are vital in initiating evidence-based strategies.
Further research should encompass the potential sustainable solutions to safeguard college students’ mental well-being during such health crises. Notably, after learning the practical existence of a social problem, the next step must be seeking a solution. The key lesson from the available research is that the community must find effective strategies to respond to future pandemics.
The need for an effectively coordinated integrative global health sector to handle future health crises in groups, including college learners, is inarguable. Therefore, besides the vital implications of the COVID-19 pandemic on students’ psychological and mental welfare, education and community stakeholders can prepare adequately to counter future destabilization.
References
Chriscaden, K. (2020). Impact of COVID-19 on people’s livelihoods, their health, and our food systems.
Coughenour, C., Gakh, M., Pharr, J. R., Bungum, T., & Jalene, S. (2020). Changes in depression and physical activity among college students on a diverse campus after a COVID-19 stay-at-home order.
Lee, J., Solomon, M., Stead, T., Kwon, B., & Ganti, L. (2021). Impact of COVID-19 on the mental health of US college students. BMC
World Health Organization. (2021). The impact of COVID-19 on global health goals.
If you enjoyed reading this post on the impact of COVID-19 on college students, I would be very grateful if you could help spread this knowledge by emailing this post to a friend, or sharing it on Twitter or Facebook. Thank you
Kant’s Autonomy in relation to Drug Use Assignment – Morality and ethics are like a reflection of what we believe where moral laws and tend to refine or improve what we believe in. In most societies, justifying the need to limit the use of drugs is always controversial as some people are of the view that they should be left to choose what is good for their bodies and what is not (Smith, 2002). Therefore, the legalization of drugs in some societies has been mandated on the grounds of helping people achieve their autonomy or exercise liberty.
However, there are always consequences associated with engaging in drug-taking activities where it is noted that drugs directly affect the self while indirectly impacting society (Altman, 2011). Therefore, the arguments for regulating the intake of drugs is centered around the consequences of taking drugs and the intentions to take drugs as well as the autonomy of the human being. This brings the need to ask questions, is it right to regulate the use of drugs? Does an individual’s ability to choose limited through legislation, is this enslavement?
According to Kant, the individual or a person has a certain dignity that requires an individual’s respect. Kant notes that the reason showing why people are sacred stems from the idea that we are rational humans who can use logic (Altman, 2011). Kant also notes that human beings are autonomous beings meaning that one can act and choose freely. In this case, autonomy focuses on an individual’s ability to govern the self.
This school of through is therefore based on the ability to focus on the self as a way of determining what is moral and immoral instead of being influenced by the injunctions of other people (Kant’s Moral Philosophy (Stanford Encyclopedia of Philosophy), 2016). This, therefore, entails self-governance where an individual looks the self and hence pursuing the course of action that benefits the self despite the moral beliefs and norms revolving around the choice.
Further to that, according to Kant, an individual’s autonomy is compromised when the individual cannot make a decision individually. This is when an external body or external factors influence them may fail to be autonomous since the true self does not exist at this moment (Altman, 2011). For example, a child may have the inability to be autonomous as well as the disabled people or an oppressed individual as they may be having the inability to become autonomous.
This, therefore, presents autonomy as the ability to be fully aware of having authority over individual actions. Kant, therefore, calls upon the need to let the individual free will be the major guiding principle towards decision making rather than letting the socially developed principles and or laws and hence determining what is moral (Kant’s Moral Philosophy (Stanford Encyclopedia of Philosophy), 2016).
In this case, people should be guided by the maxims which they choose to abide by where such maxims can be regarded as universal by any being. Kant further notes that our emotions and subscriptions are external to the development of the will and therefore, they should not play a role in determining the ability to self-regulate (Altman, 2011).
Kant’s Autonomy
In other words, Kant means that our feelings, habits, the emotions that we develop do not contribute towards the achievement of autonomy are they are seen as external. However, it is important to note that the idea of free will and making personal choices does not entail being governed by no laws, but is focuses on being governed by the laws that are developed by the self. In this case, the concept of autonomy works beyond being manipulated or manipulating other beings for the sake of our good (Smith, 2002). This, therefore, means that deception and lying are not okay since if I’m being deceived or manipulated, I cannot make an autonomous decision since the decision was based on false information.
Therefore, when it comes to the issue of drug use in relation to Kant’s arguments, it can be noted that if the decision to take drugs is personal and not influenced by other external factors, it can be considered as moral by the individual (Smith, 2002). The model by Kant promotes the idea that human beings have the right to do what they deem right to themselves provided that other factors do not influence it and it does not affect other people. in fact, people with freewill have the right to undertake what they need for their bodies including engagement in drug-taking provided that it is what makes them happy. Engaging in drug-taking can be likened to engaging in sports for one’s benefit (Altman, 2011).
However, engaging in drugs because you saw another individual looking good or because you heard that taking drugs gives you a good feeling may fail to be autonomous since your decision was influenced by the arguments of others (Smith, 2002). For the person taking drugs to benefits themselves or as per their own decision can be regarded as autonomous.
Therefore, the decision to both reject and or use drugs as long as it emanates from the self can be noted as autonomous — Kant’s theory given individual liberty to determine their maxim. Therefore, if you define your maxim, you get the ability to decide what is right or wrong. We also need to ask ourselves if we are doing something for our purposes, and if the answer to this is yes, then we are doing the wrong or rather an immoral thing (Altman, 2011). This is, therefore, majorly based on the issue of consent, where if an individual is aware of all the good and bad consequences of taking drugs, but they choose the standard or the maxim within which they wish to govern their lives.
Kant’s argument on autonomy focuses on people setting their standards and determining their fate, therefore, reducing an individual’s ability to choose what is right for them to hinders their autonomy. Despite the negative consequences of drug-taking, as long as I decide self-harm, then it’s okay. This, therefore, gives one the ability to discipline themselves and do whatever they want no matter the consequences. However, we should always take into consideration the maxim or the principle within which we act upon; this is by considering whether we would want to lie to be universally accepted (Smith, 2002).
The argument focuses majorly on the intentions of the individual rather than the consequences. In this case, if the intentions to take drugs was to satisfy the self-nourishment, then the decision can be determined as moral. The consequences, which include causing social disruptions or self-harm, in this case, are not taken into consideration. Kant notes that rationality and autonomy also entail the duty to make choices to harm oneself or choose death (Finnis, 1987).
Kant’s idea is much contested due to its focus on the concept of free will in some of the areas of an individual’s life. Notably, when an individual’s actions are truly theirs, they should, therefore, not be forced by any external force, and in our lives, there are clear examples of various situations that are not autonomous (Smith, 2002). This is due to being governed by cultural laws and norms that influence the human to act in a given way, which, if let to make your own decision, you would choose to do it. Therefore, since the decision is influenced by an external factor such as a law, they fail to meet the conditions of being an autonomous decision.
That said, being compelled to make choices that do not resonate with our own beliefs and views would be enslavement. This would mean being forced to live as per another individual’s preferences, which would be unacceptable to people with different views about the use of drugs (Finnis, 1987). Therefore, people with different drug preferences cannot agree on whether it is right or wrong to use drugs.
Kant’s Autonomy and Society
Therefore, according to Kant, any time we choose to do something, we are always influenced by our desire, and therefore there is a need to govern oneself without any external interference (Smith, 2002). In this case, society cannot make decisions for an individual as people can define their standards. Governing the use of drugs would, therefore, be enslaving the people, and therefore Kant would not support the need to set government policies to regulate the use of drugs as it interferes with an individual’s autonomy (Finnis, 1987).
This is because any action that is conducted without being influenced externally had its moral worth, not because of its purpose but according to the maxim developed by the individual. Therefore, personal intentions or needs should not be weighed against the needs of the public since something good for me might be bad for the bigger population.
In conclusion, the argument concerning the need to regulate the use of drugs is a controversial one where people take different stands as per the philosophical argument they subscribe to. Looking into the consequences of drug use, it would only be good if the government uses its power to regulate the use of drugs to protect and keep safe the general population.
However, there is a need to consider the needs of the users and the ability for an individual to make personal decisions. Kant notes that there is a need to let the individual free will be the major guiding principle towards decision making rather than letting the socially developed principles and or laws and hence determining what is moral. In this case, an individual should not be forced to make decisions that do not resonate with our own beliefs.
References
Altman, M. C. (2011). Kant and applied ethics: The uses and limits of Kant’s practical philosophy. John Wiley & Sons.
Finnis, J. M. (1987). Legal enforcement of duties to oneself: Kant vs. neo-Kantians. Colum. L. Rev., 87, 433.
Kant’s Moral Philosophy (Stanford Encyclopedia of Philosophy). (2016).
Smith, P. (2002). Drugs, morality and the law. Journal of Applied Philosophy, 19(3), 233-244.
If you enjoyed reading this post on Kant’s Autonomy, I would be very grateful if you could help spread this knowledge by emailing this post to a friend, or sharing it on Twitter or Facebook. Thank you.
Post-Traumatic Stress Disorder remains one of the leading stress-related disorders and psychological issues in society today. An understanding on to the treatment of and the management of the disorder for those with and prone to the problem is necessary. A lot of research, and shown in the literature review below, has explored the specific areas of interest and the common strategies used by psychologists, medical doctors and other professionals in the treatment of and management of Post-Traumatic Stress Disorder.
It, however, remains a challenge to find and implement an integrated approach towards Post-Traumatic Stress Disorder treatment and management. It is the labor of this research review to bring together articles and ideas from empirical reports and researches on managing and treating Post-Traumatic Stress Disorder with an aim to create an integrated approach towards the management and treatment of the disorder.
The research recognizes the diversity of possible remedies towards Post-Traumatic Stress Disorder and seeks to bring together four out of the many possible approaches for a program that offers effective remedies for Post-Traumatic Stress Disorder. It recognizes that effective management and treatment of Post-Traumatic Stress Disorder will require a practising psychologist to look beyond the symptoms he or she can see and consider the external inputs to the individual.
As a conceptual framework, therefore, effective management of and treatment for Post-Traumatic Stress Disorder is equal to successful identification of the external factors affecting, influencing and worsening Post-Traumatic Stress Disorder plus the internal factors affecting, influencing and worsening the Post-Traumatic Stress Disorder in the individual. This proposition includes several faces about Post-Traumatic Stress Disorder. First, the disorder is a non-hereditary one and the person suffers Post-Traumatic Stress Disorder in the course of their life.
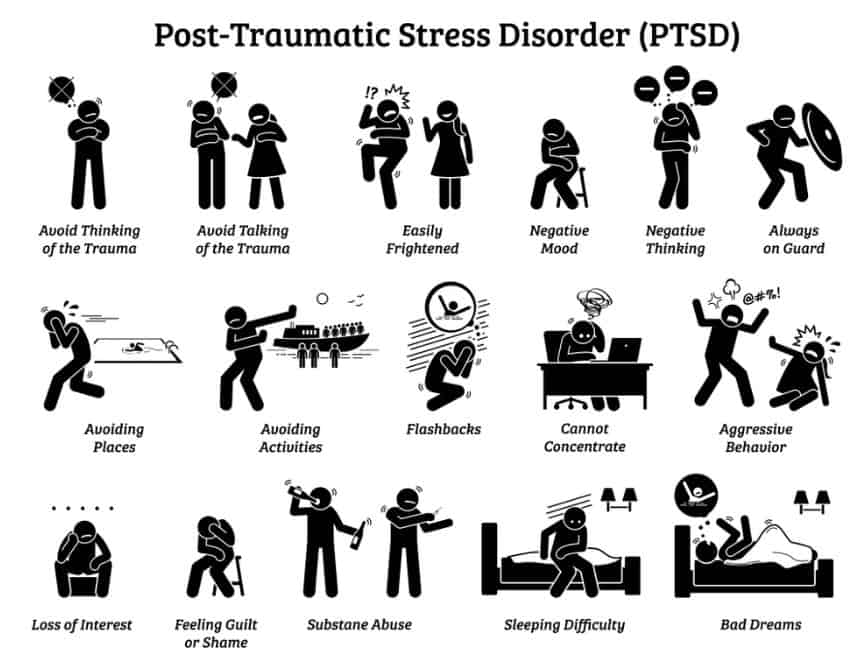
This is triggered by traumatic experiences such as rape, domestic violence, war and other terrible occurrences such as terrorism and molestation. These are all external factors which often are out of control of the person will. They infiltrate the person’s peaceful course of life from outside and are often unpredictable. They can be summed up as external pressures that lead to Post-Traumatic Stress Disorder. Secondly, the disorder, once it takes its seat in the person’s life, causes several psychological and psychosocial changes in the individual that alter the general behavior of the person and especially, their perception of various stimuli.
The person starts to associate different stimuli with the trauma-related events that they witnessed a long time ago and therefore subjects the individual to a troubled life. lastly, the person being addressed and who is the Post-Traumatic Stress Disorder patient lives in a society of human beings who, from time to time, interact with the patient at different levels. Such interactions will cause various reactions by the society or the individual.
This research will identify the third class of elements part to a Post-Traumatic Stress Disorder patient effective intervention program as the secondary factors. The level or ability of such a society in handling depression and especially, Post-Traumatic Stress Disorder, will determine at a large scale, the trajectory of the individual towards or away from recovery. This is because society will be the support state of the patient.
Addressing Post-Traumatic Stress Disorder
In developing the program and with a view to a multifaceted approach to managing and treating Post-Traumatic Stress Disorder, this review adopts the framework: effective treatment of Post-Traumatic Stress Disorder = addressing external factors + internal factors + external secondary factors. To effectively address the factors, the treatment for Post-Traumatic Stress Disorder will acknowledge the need to include four domains of parties and knowledge necessary for a holistic person, where holistic means addressing all the issues party to Post-Traumatic Stress Disorder and necessary for sustained relief and recovery from the disorder.
As such, the research identifies four main domains of psychology that are important for integration in the treatment of and management of Post-Traumatic Stress Disorder. The domains include the psychological practitioners on the clinical, cognitive, social and rehabilitative. The four are chosen based on their contributions towards a holistic personal focus by psychological practitioners on the clinical, cognitive, social and rehabilitative treatment and management programs, which may take place at the hospital and the home.
There is a seamless connection between the four domains highlighted above and which will be used in the literature review. First, the patient needs drugs that are used to alleviate the deconstructive thoughts and flashbacks and often, the false sense of danger of alarm with patients with psychological practitioners on the clinical, cognitive, social and rehabilitative. The program would include a clear and accurate clinical identification of the problem through careful consultation with a doctor, more so, a psychologist or a clinician.
This is usually the first step in attending to a patient of any kind as long as they can respond to the consultant’s investigation unbiased. Upon the identification of the problem, there is a need for pharmaceuticals to identify the right drugs, if there are any, to counter the traumatic ideation and experiences or memories of the patients, toning down the symptoms of the disorder. Above that, medical science should establish science-based, theoretical and clinical knowledge perspective in relieving, preventing and understanding human psychological ill-health. on the other hand, there is the need to manage the social circles of the patents in such a way that the circles promote, rather than worsening, the recovery process of the patients. The social domain calls for the acts of those around the victim to be controlled so as to produce pro-healing efforts for the victim.
Social psychology studies how people’s acts affect those of others, in our case, the wellbeing of people with Post-Traumatic Stress Disorder. Upon understanding the clinical and social inputs necessary for the whole recovery of the Post-Traumatic Stress Disorder patient, the effective program should consider understanding and attending to primary diseases or states of well-being that promote Post-Traumatic Stress Disorder. An example is spinal and brain injury.
Such patients are more likely to suffer from Post-Traumatic Stress Disorder than any other healthy person. The connection between the chronic diseases and the disorder will be studied carefully with a view to a better management strategy for such patients. A proactive means to curbing the possibility of Post-Traumatic Stress Disorder arising from or among such parents will be reviewed with a view to using rehabilitative psychology as a domain and input to managing the disorder. To yield the best results and for an effective therapy for persons with the disorder, cognitive psychology will be applied.
This psychology includes, among other things, managing the cognitive behavior, including perception, of the Post-Traumatic Stress Disorder patient. It has been shown to be one of the most effective means to treating Post-Traumatic Stress Disorder and other research shows that cognitive behavioral therapy works very well, most effectively, when combined with injunction interventions such as eye movement desensitization and reprocessing. Ultimately, the four domains will rely on each other for the successful treatment of and management of the disorder.
While these domains have been used before, the integration of the four for a single program aimed at effective treatment of post-traumatic stress disorder has not been recorded. It is the burden of this review to show the critical need to have the disorder approached from different angles, hence the development of this literature review pending deeper research thereafter.
This literature was chosen on basis of their primacy and direct address to the various domains as well as their verifiability, coming from an authentic and official library. In so doing, the literature review hypothesizes that only an integrated approach to managing Post-Traumatic Stress Disorder would fully address the growing prevalence of Post-Traumatic Stress Disorder in America.
Discussion
Post-traumatic stress disorder is as a result of the interacting external and internal factors that are related to or associated with the first instance of the traumatic experience and sustain or repress subsequent manifestations of trauma. Specifically, it is a psychological disorder regulated by factors which the person can control and others that he can’t control. Therapy ought to, therefore, recognize the different angles and interventions necessary for Post-traumatic stress disorder treatment for holistic treatment.
Experts consider a holistic approach to health and wellness as the optimal approach, given the side effects and resultant disorders and symptoms of ill-health or anti-social behavior that can result from psycho-social disorders. To them, treating the identified disease without paying attention to the external and internal climate encouraging the disease or disorder would only offer short-term reprieve but leaving nothing for the long-term. Without the holistic approach to ill-health, therefore, treatment would be ineffective in psycho-social disorder (Auxier, Farley & Seifert, 2011).
Clinical Psychology Domain
The first step for an already exposed population ought to be an investigative approach to identify those with post-traumatic stress disorder symptoms and those who do not. Cognitive approaches can be used and this may include a simulation of the suspected event that is feared to have caused post-traumatic stress disorder as well as clinical trials or measures. Clinical psychology, as the term denotes, interests itself with the science-based theoretical and clinical evidence approaches to relieving human suffering from diseases.
In the case of post-traumatic stress disorder and in psychology, it includes the active interrogative, investigative and documentation process to identifying people with or without post-traumatic stress disorder. It seeks to understand ill-health from an evidence point of view. Integrated health management calls for thorough investigations to identify a problem before working on a solution, the reason why clinical psychology comes next to none of the four interventions and domains of psychology in this integrated literature review.
In a study carried out by Ferry, F., Bunting, B., Murphy, S., O’Neill, S., Stein, D., and Koenen, K. in 2014, the authors reported that many issues of violence precipitated post-traumatic stress disorder in Northern Ireland, a zone potential of violence and civil threats. They noted that the population sample of 4340 subjects revealed possibilities of post-traumatic stress disorder upon children and adult exposure to the death of a close friend or a loved person such as children, parents or a sibling, partner violence or threat to a partner or close friend can lead to post-traumatic stress disorder.
These are common occurrences in our societies with people getting assaulted with freehand, crude weapons or guns in every corner. The church shootings, school shootings and street racialized shootings, as well as domestic gun violence in America, expose our children and loved ones to health stressors akin to the situation in Northern Ireland. The implication of their study is that such people as having witnessed assault or violence by a close friend or a loved one need to be screened for, on a going basis, post-traumatic stress disorder among other disorders.
Those found with the slightest of symptoms for post-traumatic stress disorder should be attended to with counselling and where necessary, with cognitive behavioral therapy and eye movement desensitization and reprocessing programs among other interventions.
While programs for therapy and interventions among people with post-traumatic stress disorder would be an effective proactive means to reducing and eliminating post-traumatic stress disorder in the population, there are several internal factors that hinder the quick recovery from the disorder. Seligowski, A. V., Miron, L. R., and Orcutt, H. K. (2015) identify self-compassion as a positive factor in reducing trauma and traumatic manifestations for persons with post-traumatic stress disorder.
Those with high levels of self-compassion and self-pity are more likely to recover and cooperate than those who have reduced self-compassion. This discovery means that cognitive behavioral therapy should include enhancing the individual self-awareness of their condition and their self-compassion, which, predictably, should enhance their means to recovery. The results indicate a need to further research on the other personal emotional factors that could contribute to faster recovery.
However, clinically critical empirical results from two researches show that drug abuse and substance abuse, as well as psychological inflexibility, are two factors that lead to prolonged post-traumatic stress disorder and irresponsiveness in treatment. The first study indicates that psychological flexibility is a positive factor in the treatment of post-traumatic stress disorder while inflexibility is a negative contributor. Those who are willing to flex their opinions and views concerning themselves and concerning the encounters they went through are more likely to recover than are those who are inflexible.
Again, high inflexibility is a predictor for increased post-traumatic stress disorder manifestation (Meyers et al, 2018). Clinicians and psychologists ought to understand this and similar factors that make recover from post-traumatic stress disorder difficult among patients and develop programs that seek to increase the psychological flexibility of patients and persons likely to be or already exposed to post-traumatic stress disorder. On the other hand, Reisman (2016) associates’ drug and substance use with post-traumatic stress disorder, noting that in a study including US war veterans, the majority of them were drug abusers.
Drug abuse, he notes further, can lead to a worsening state of post-traumatic stress disorder, given that the drugs can lead to further depression and impaired judgment, which can, in turn, lead to suicidal ideation. Among the drugs most commonly abused by war veterans are alcohol and cocaine as well as cigarette, all of which have side effects and withdrawal effects as well as cause ill-health in large contents. Still, drug abuse can hinder cooperation between a therapist and the patient and the intervention program should understand the drug history of the patient as well as their current drug abuse status.
Effective intervention, therefore, would start by preventing drug abuse among persons exposed to traumatic war experiences as these are precipitates for further and worsening post-traumatic stress disorder.
As a breakthrough in post-traumatic stress disorder management and treatment, there are drugs that have been found to work best in addressing the symptoms of post-traumatic stress disorder and which ought to be used as the initial strategy for treating the disorder. In pharmacotherapy addressing post-traumatic stress disorder, drugs that act directly on the serotonergic systems are effective when used for a long period.
They actively suppress the trauma thoughts and flashbacks that cause the symptoms for the disorder and thus intervene for a change in the post-traumatic stress disorder experience of the person. The drugs include but are not limited to monoamine oxidase inhibitors and selective serotonin re-uptake inhibitors (Sauer & Bhugra, 2001). The former includes the drugs used to inhibit monoamine oxidase A or B or both, abbreviated as MAO-A and MAO-B. the two monoamine inhibitors work against depression by functioning as strong anti-depressants and throwing the depressed out of panic and social phobia. As the person becomes less panicked and more sociable, the post-traumatic stress disorder symptoms are mitigated.
Likewise, the selective serotonin reuptake inhibitors are active and powerful antidepressants, functioning by increasing the extracellular amounts of neurotransmitter serotonin through reduced reabsorption or reuptake into the presynaptic cell. This lowers depression, thus, countering the depressive effects of post-traumatic stress disorder. This calls for, however, a patient and intelligent examination of the progress and a combination with conservative therapy strategies such as cognitive behavioral therapy and the eye movement desensitization and reprocessing as the length of time for the drug administration is not a direct predictor or factor for the speed of or level of recovery.
Therapy, therefore, should concentrate on eliminating the psycho-social instabilities through a combination of pharmacological and psychological therapies such as eye movement desensitization and reprocessing and cognitive behavioral therapy (Gutermann, Schwartzkopff & Steil, 2017).
Social Psychology Domain
Social psychology engages itself with the manner or processes and reasons why one person’s acts influence or affect the other. In this domain and in line with Post-traumatic stress disorder, there are several social environment factors that would hinder the full recovery of the Post-traumatic stress disorder patient, even when effective drugs have been provided and complete therapy or recovery has been foreseen. first, physicians and counsellors must understand that in order to design a therapy program for a person suffering from Post-traumatic stress disorder and whose impact event that led to the disorder was due to an encounter they went through, the intensity of the disorder is as often directly proportional to the period of time or intensity of exposure they had with the traumatic event.
Chou et al (2011) studied a group of 1966 children who had post-traumatic stress disorder arising from physical abuse by their relatives or a close friend at home. The authors noted that the longer the children, all of whom were from grades 4 to 8, expressed symptomatic PTDS relative to their period of exposure. They had severe peri-traumatic subjective reactions as compared to those exposed for a short time.
This is because during the time of exposure, the traumatic events continue to register in the persons conscious and subconscious mind and their somatic cells end up relating every repeating event of trauma to the former, and subsequently to the first encounter, growing a bolder association of the stimuli and the results of their experience. This implies that a patient who experienced traumatic events for a whole decade should be given more attention, subject to their resilience and response to therapy, that one who has just had a day’s experience.
The social approach is important because while the research indicates a direct relationship between the time of exposure of the patient to the traumatic event, research also finds that intimate partner abuse can lead to post-traumatic stress disorder with a sample of 128 African-American women population, the authors noticed that the strategies the women would choose would determine whether or not they will end up in post-traumatic stress disorder and if yes, to what extent.
The authors noted that both psychological non-physical and physical abuse leads to Post-Traumatic Stress Disorder. However, they noted that non-physical psycho-social abuse was more prevalent as compared to the physical abuse (Mills, Hill & Johnson, 2018). What this means is that for a woman living with an abusive woman or a man living with an abusive woman as a husband and wife, there are chances that either party, the aggrieved one, will suffer post-traumatic stress disorder. Given the home setting and husband-wife relationships and the time the two spend together, there will always be prolonged exposure to the trauma-causing abusive events to the abused party.
A wife may spend a prolonged life with an abusive husband and vice versa without opting out of the relationship. Gain, the one party can take advantage of the intimate relationship to advance their ill-aimed mistreatment or violence towards their spouses in an America where husband-wife wrangles and tensions are always a probability. This consists of Runyon, Deblinger & Steer (2014) who noted in their research that parental abuse would lead to post-traumatic stress disorder. In their case, if one parent is caring and comforting while the other one is abusive or neglecting, such a mismatch wouldn’t cancel the probability for Post-Traumatic Stress Disorder.
If the one causes the children to go through hellish experiences while the other, probably the mother, creates an encouraging and positive environment for the growing children, they will experience Post-Traumatic Stress Disorder still. The pampering of one parent cannot, therefore, reverse the damages caused by the other. In their review, the authors noted that the effects brought about by the abusive parent were independent with the love shown by another, meaning that the parent will inflict the son or daughter with trauma-causing experiences that cannot be compensated through love and care from another parent.
As such, proactive prevention of post-traumatic stress disorder includes the training for parents to actively provide the right environment for their children and for relatives of adults suffering the disorder to eliminate cases of inhumane treatment by other family members in order to provide an environment that discourages the development and persistence of post-traumatic stress disorder.
Also, Oravecz et al note in their study that post-traumatic stress disorder is not a preserve for persons working in war-torn areas or terror zones, accident occasions and other fatal experiences. They argue and research the prevalence of post-traumatic stress disorder among persons working in Slovene medical emergency units.
The authors realize that post-traumatic stress disorder is common among staff working in ICU and other critical incidence areas in the hospitals, results which can be generalized across the medical profession and the hospital environment all over the world. It is needful, in the spirit of a proactive preventive approach towards post-traumatic stress disorder, to cover such staff as are working in areas that expose them to traumatizing conditions of disease and human sufferings which cause flashbacks among clinical and medical officers. These include all people dealing with broken or missing human limbs out of accidents and other emergencies referred to hospitals and being attended by medical and support staff. One such a program for self-care and organized human resource care ought to be continuous counselling and retraining to cope with and withstand the many cases of critical illnesses and cases of accidents witnessed by the medical officers.
In their studies, Zulueta (2007 and Evans et al (2009) conclude that indeed, persons exposed to September 11, 2001, World Trade Center disaster and persons witnessing mass violence had similar outcomes; they both suffered post-traumatic stress disorder. Zulueta notes that mass violence leads to mass detachment and separation between children and their parents as well as relatives and subject the witnesses to inhumane conditions which trigger trauma symptoms.
Such witnesses may need immediate attention, a subject that delves to the preventive program of post-traumatic stress disorder intervention methods. On the other hand, 842 people who had been involved in the world trade Centre attack showed that those who had any forms of disability were more prone to post-traumatic stress disorder compared to those who didn’t. The two studies outline the need for witnesses of mass violence or terror attacks should be attended to proactively with counselling sessions and especially, those who have any forms of disability, as they are more likely to develop post-traumatic stress disorder than those who are whole and healthy.
The September 11, 2001 World Trade Center report reveals that these categories of individuals are more likely to suffer post-traumatic stress disorder because of their limitations in movement as well as their inability to flee from the scene which subjects them to more horrible conditions of susceptibility as compared to their fellow workers, friends or family members without disabilities.
Rehabilitative Psychology Domain
Understanding the social demographics prone to the likelihood of developing post-traumatic stress disorder is as important as is the understanding of cases where the disorder is likely to develop among people undergoing medical care or critical treatment. Rehabilitative psychology deals with the psychological processes among people undergoing medical treatment.
These are being rehabilitated or treatment for serious injuries such as cancer, spinal injury, brain injury among other excruciating diseases. People with such illnesses are likely to suffer post-traumatic stress disorder due to the memories and/or nightmares they experience. Their therapists ought to understand the challenges they face, the manifestations they have which are symptomatic of post-traumatic stress disorder and how to address them before they advance to a more serious case of post-traumatic stress disorder.
The likelihood that a worker who witnessed fatalities at the place of work will develop Post-Traumatic Stress Disorder is high in the US as well as any other place in the world. In the United Steelworkers research, about 26 percent reported Post-Traumatic Stress Disorder symptoms while another 21 percent reported subthreshold Post-Traumatic Stress Disorder symptoms (Blake et al, 2014). Blake also notes that such people may benefit if a program for counselling and continuous screening was availed for them and they would be in less danger of developing post-traumatic stress disorder symptoms.
Blake and company used a representative population sample of 89 individuals. It is not in industries and factories where accidents are likely to occur where workers are exposed to the development of post-traumatic stress disorder. In a separate study by Abeyasinghe and other researchers in 2012, the authors find that people who had been in the military and had lost either one or more limbs or body parts or had suffered a spinal injury in the course of their work developed a post-traumatic stress disorder. Such statistics show how often employees in the military are likely to suffer post-traumatic stress disorder, given the many chances of amputations and accidents leading to spinal injury among the men in uniforms.
During their rehabilitation programs, they are prone to flashbacks of the events leading to their injuries and loss of their limbs or the amputation, thus, suffering from post-traumatic stress disorder symptoms. This is akin to the experiences of industrial workers witnessing or being affected by industrial accidents, as studied by Blake et al (2014). Similarly, Wisco et al (2014) carried out a study that involved people who had served in the Afghanistan war as US veterans. In the study, the authors sought to establish the relationship between their experiences and traumatic brain injury, post-traumatic stress disorder and suicidal ideation.
Suicidal ideation is a subset of post-traumatic stress disorder but a symptom of other psychological and psychiatric disorders. They found that among the veteran’s study which accounted for 824 males and 825 females, there was an increased risk of post-traumatic stress disorder and suicidal ideation. These findings point to the devastating results of traumatic experiences by war veterans and their younger ones, those already in the battlefields through the army and other counter-terrorism programs. They also indicate the need for more proactive programs to attend to survivors of war, not just in the battlefield marshal’s category, but also among volunteers and good Samaritans who risk their lives to save perishing souls in war areas.
Bahraini et al (2013) studied a population of people living with and undergoing treatment for traumatic brain injury with an intention to establish the relationship between those undergoing rehabilitation for brain injury and post-traumatic stress disorder. The authors realized that all the secondary data used, with 16 different and diverse sources screened, pointed to the increased development of post-traumatic stress disorder symptoms among such patients.
Specifically, suicidal ideation was marked as prevalent ideation among patients undergoing treatment for brain injury caused by traumatic injury. Such populations require active and proactive screening for post-traumatic stress disorder, given the high chances of the development. In the same manner, people suffering from spinal cord injury were all found to have increased chances of suffering post-traumatic stress disorder (Otis, Marchand & Courtois, 2012). In a similar but separate study, Caspi and a group of researchers noted that the memory of the traumatic event is associated with increased risk for Post-Traumatic Stress Disorder.
While people suffering from critical brain and spinal injury are likely to have flashbacks of what happened, their memory of such events would lead to higher chances and prevalence of post-traumatic stress disorder during and after their rehabilitation. The study of 120 subjects showed that those who remember the events will suffer post-traumatic stress disorder while those who don’t remember them will not (Caspi et al, 2005).
These findings, combined with the study on persons who got amputated on either or all limbs, reveals the importance of proactive intervention by counselors to persons or groups of persons undergoing brain, spinal or amputation surgery and treatment. The treatment part is important but is inadequate if the environmental factors in terms of memories will not be addressed. This calls for programs such as cognitive behavioral therapy and eye movement desensitization and reprocessing which help to rebuild the narratives or memories of the events to friendlier versions.
Cognitive Psychology
Having identified the factors leading to, precipitating and contributing to persistence of traumatic flashbacks and other post-traumatic stress disorder manifestations or symptoms, an effective program ought to consider the cognitive behavior and possible approaches to reframing or refashioning the cognitive processes of the patients and people likely to suffer from post-traumatic stress disorder due to their exposure to diverse situations.
Such factors include how a person views himself once they have post-traumatic stress disorder and the value, they attach to themselves. Keshet, H., Foa, E. B., & Gilboa-Schechtman, E. (2018) shows through empirical research that indeed, women who are victims of traumatization suffer from a negative self-image. Management of post-traumatic stress disorder, therefore, should focus on reversing the negative self-perception of women and reconstructing positivity through the cognitive behavioral therapy ascertained as an effective intervention for long-term recovery. Also, women who are repeatedly teased suffer from post-traumatic stress disorder, a situation that is common among most societies where wife battering and demeaning is still active and where women suffer direct and indirect teasing from fellow women or workers.
Such an understanding should help cognitive therapists to manage post-traumatic stress disorder among such clients by counselling for teasing and similar exposures. Kishimoto, Goto and Hashimoto (2014), however, notes that such negative effects can be reversed using drugs such as gabapentin and lamotrigine. The drugs help to mitigate painful experiences as well as unpleasant experiences resulting pressure from teasers and other manipulative experiences from peers and men who tease women, as shown by Kishimoto, Goto and Hashimoto.
Prolonged exposure therapy has been recommended as an effective pro-cognitive strategy to address post-traumatic stress disorder among the worst-hit and mild patients, posing as one of the means through which psychologist can address post-traumatic stress disorder (Kumpula et al, 2017). Again, the method can be combined with other effective programs such as cognitive behavioral therapy for effectiveness and efficiency, noting that drugs help to mitigate for the short-term while cognitive behavioral therapy, eye movement desensitization and reprocessing and prolonged exposure normalizes the experiences, reduces the phobia and intervenes for a post-traumatic stress disorder.
In another research, Ogle, Siegler, Beckham and Rubin (2017) find that neuroticism increases post-traumatic stress disorder symptom severity by amplifying the emotionality, rehearsal, and centrality of trauma memories. Neurotic persons, that is, people with high scores in the personality trait measures using the big five personality traits, are more prone to post-traumatic stress disorder as the status makes one more easily depressed and subject to anxiety and depression.
The cognitive behavioral therapy, as such, ought to focus on taming neuroticism for such individuals, meaning that the psychologists need to understand the person’s character profile. This, according to Reid (2005), should include active mediation and intervention for the memory reprocessing and reconstruction of the actual experiences through flashbacks. Also, active mediation for insomnia and nightmares, which brings back the old experiences as if they were fresh (Reid, 2005), ought to be addressed to improve both sleep quality and the speed of recovery from post-traumatic stress disorder (Krakow et al, 2001).
Critique
The literature used in this review is an integration of various approaches to research on managing post-traumatic stress disorder using the four domains, that is, clinical, rehabilitative, social and cognitive psychology. The four areas are pre-selected domains, based on the need to approach therapy for post-traumatic stress disorder as a psychological problem that includes various external and internal factors either repressing or enhancing the disorder.
The data from the four domains and the literature reviewed contains results from empirical and scholarly studies by authors using sample studies, giving the results credibility and reliability as an ideal resource portfolio for post-traumatic stress disorder research. the literature fully represents the four domains in terms of both active and proactive interventions as well as internal and external factors affecting the recovery and extent of post-traumatic stress disorder. The use of empirical data and studies enhances generalizability, given that they derive their conclusions from representative samples of subjects using experimental and explorative studies.
They derive their authority from the experimental, explorative and empirical nature, relating real-life experiences of war veterans and women subjected to teasing, domestic violence, children subjected to traumatic experiences such as war and accidents among other experiences, and clinical research in drugs and other therapies for a post-traumatic stress disorder. The studies, nevertheless, do not reveal an outright or evidence-based integration and this is why the literature review aims to explain the need for integrated management of post-traumatic stress disorder.
The pieces of evidence raised from the literature matches the claims made in the introduction that post-traumatic stress disorder needs an integrated approach towards management and therapy since it is a multi-factor disorder. The APA ethical principles of psychologists and code of conduct require express permission from the subject’s party to human-subject studies and these have been followed in the majority of the literature above which required human involvement as subjects. The standards were almost uniform across the literature with individuals participating in all the studies doing so upon personal consents from a person with the capacity to give consent, that is, free from any perceptual bias.
Synthesis – Post-Traumatic Stress Disorder
The research review explains, in much detail, the integration of diverse means of treating and managing post-traumatic stress disorder. Chou, Su, Wu and Chen (2011) notes that among other things, the time exposure affects the recovery process while the drug use period doesn’t affect the effectiveness of the treatment. This is necessary for therapists given that the post-traumatic stress disorder problem calls for both pharmacological and conservative methods of therapy. In this case, an integrative approach would call for both drug and non-drug-based therapy programs personalized for the specific cases, given that different groups of individuals have different internal and external factors affecting their ability to recover and the recovery process.
Also, understanding the internal and external environmental inputs should come first in mediating for a post-traumatic stress disorder. This calls for the need to investigate further how the four domains can be effectively applied to fasten and sustain therapy. In the literature, again, cognitive behavioral therapy, eye movements desensitization and reprocessing have been noted as critical approaches towards the treatment and management of post-traumatic stress disorder with a careful drug administration to suppress depression and ignite sociability.
Notably, the literature reveals that understanding the precipitates to post-traumatic stress disorder, the factors that enhance post-traumatic stress disorder, the conditions that suppress post-traumatic stress disorder, the drugs that inhibit the disorder symptoms and the means to intervention for the disorder are all to be jointly addressed for a sustainable therapy for a post-traumatic stress disorder. I propose that a systematic management program ought to include the clinical, empirical and environmental understanding of the individual cases. This ought to include both the stressors the individual is currently facing, the events that triggered the traumatic manifestation and the symptoms party to the specific case, including the drugs most effective in the inhibitory process, in order for a holistic intervention and optimal results to be realized.
The psychologist, again, should seek to understand the social factors, the cognitive factors and therapy options, the clinical evidence and the rehabilitation experiences and voids for people with post-traumatic stress disorder in order to effectively handle the client from an empirical or informed point of view. Finally, effective post-traumatic stress disorder prevention, treatment and management ought to include different players which include pharmacologists, psychologists, and clinicians.
Conclusion
As the literature above has revealed, post-traumatic stress disorder continues to be one of the most challenging mental issues in the world today. While the problem has attracted much research and inquiry into effective combinations of conservative methods and drug-based therapy programs, there is no clear research as to how cognitive behavioral therapy, eye movement desensitization and reprocessing can be combined with drugs to ensure faster and more effective therapy.
Still, there is a need for a deeper understanding of the interacting factors leading to prolonged or sustained post-traumatic stress disorder symptoms among people who have experienced war, industrial accidents, violence and child abuse among other issues of mental torture or trauma. In so doing, the social psychologist needs to participate in developing a good and supportive external environment for the patient to recover.
This may include counselling the caretakers of the patient to avoid such events and stimuli as will remind the person of their traumatic experiences and cognitive behavioral therapy secondary care activities that include physical exercise and social activities. The cognitive psychologist will need to reframe the individual’s self-perception or help the victim to normalize their traumatic experiences through exposure therapy, cognitive behavioral therapy and eye movement desensitization and reprocessing therapy techniques, all of which aim at healing the patient from the short and long term effects of post-traumatic stress disorder as well as the clinicians to effectively identify post-traumatic stress disorder symptoms in patients and evidence-based interventions for post-traumatic stress disorder clients.
Such an approach, that is, an integrated approach to post-traumatic stress disorder management using multifaceted psychological approaches, as explained by the research from the four domains of rehabilitative, clinical, social and cognitive psychology, would make post-traumatic stress disorder treatment and management more effective and efficient. It would also make psychologists more effective and knowledgeable, alleviating the health concerns arising from post-traumatic stress disorder-prone populations such as the survivors of war and military strikes as well as the victims of Karen and Burma among other like-stricken areas.
There are however questions to be answered going forward. First, what combinations of the conservative techniques of cognitive behavioral therapy, eye movement desensitization and reprocessing and exposure therapy work best and why? The answer to this question would grant psychologist an informed database to rely on for empirical evidence in conservative non-drug-based therapy for post-traumatic stress disorder treatment.
Secondly, what would be the best approach for equipping psychologists with the knowledge necessary to implement the four domains in developing a single integrated program for post-traumatic stress disorder therapy? This answer ought to lead the research to the development of a knowledge approach, one in which the psychologist is supposed to understand various modules concerned with the post-traumatic stress disorder integrated management and therapy in order to understand the pharmacological, social and cognitive strategies for an optimal interventional program.
Lastly, the question as to the cost implications of an integrated approach to post-traumatic stress disorder management and treatment arises, seeing that the more knowledgeable the psychologist ought to be, the higher an asset he or she becomes and the more expensive he is likely to become. Also, the more attention is given to individual clients, the more expensive it is likely to be. These are some of the questions that need to be answered alongside the proposition for an integrated approach to post-traumatic stress disorder management.
References
Abeyasinghe, N. L., de Zoysa, P., Bandara, K. M. K. C., Bartholameuz, N. A., & Bandara, J. M. U. J. (2012). The prevalence of symptoms of Post-Traumatic Stress Disorder among soldiers with amputation of a limb or spinal injury: A report from a rehabilitation centre in Sri Lanka. Psychology, health & medicine, 17(3), 376-381.
Auxier, A., Farley, T., & Seifert, K. (2011). Establishing an integrated care practice in a community health center. Professional Psychology: Research and Practice, 42(5), 391.
Bahraini, N. H., Simpson, G. K., Brenner, L. A., Hoffberg, A. S., & Schneider, A. L. (2013). Suicidal ideation and behaviours after traumatic brain injury: a systematic review. Brain Impairment, 14(1), 92-112.
Blake, R. A., Lating, J. M., Sherman, M. F., & Kirkhart, M. W. (2014). Probable PTSD and impairment in witnesses of work-related fatalities. Journal of loss and trauma, 19(2), 189-195.
Caspi, Y., Gil, S., Ben-Ari, I. Z., Koren, D., Aaron-Peretz, J., & Klein, E. (2005). Memory of the traumatic event is associated with increased risk for PTSD: A retrospective study of patients with traumatic brain injury. Journal of Loss and Trauma, 10(4), 319-335.
Chou, C. Y., Su, Y. J., Wu, H. M., & Chen, S. H. (2011). Child physical abuse and the related PTSD in Taiwan: The role of Chinese cultural background and victims’ subjective reactions. Child abuse & neglect, 35(1), 58-68.
de Zulueta, C. F. (2007). Mass violence and mental health: Attachment and trauma. International Review of Psychiatry, 19(3), 221-233.
Evans, S., Patt, I., Giosan, C., Spielman, L., & Difede, J. (2009). Disability and posttraumatic stress disorder in disaster relief workers responding to September 11, 2001 World Trade Center disaster. Journal of clinical psychology, 65(7), 684-694.
Ferry, F., Bunting, B., Murphy, S., O’Neill, S., Stein, D., & Koenen, K. (2014). Traumatic events and their relative PTSD burden in Northern Ireland: a consideration of the impact of the ‘Troubles’. Social psychiatry and psychiatric epidemiology, 49(3), 435-446.
Gutermann, J., Schwartzkopff, L., & Steil, R. (2017). Meta-analysis of the long-term treatment effects of psychological interventions in youth with PTSD symptoms. Clinical child and family psychology review, 20(4), 422-434.
Keshet, H., Foa, E. B., & Gilboa-Schechtman, E. (2018). Women’s self-perceptions in the aftermath of trauma: The role of trauma-centrality and trauma-type. Psychological trauma: theory, research, practice and policy.
Kishimoto, A., Goto, Y., & Hashimoto, K. (2014). Post-traumatic stress disorder symptoms in a female patient following repeated teasing: treatment with gabapentin and lamotrigine and the possible role of sensitization. Clinical Psychopharmacology and Neuroscience, 12(3), 240.
Krakow, B., Johnston, L., Melendrez, D., Hollifield, M., Warner, T. D., Chavez-Kennedy, D., & Herlan, M. J. (2001). An open-label trial of evidence-based cognitive behavior therapy for nightmares and insomnia in crime victims with PTSD. American Journal of Psychiatry, 158(12), 2043-2047.,
Kumpula, M. J., Pentel, K. Z., Foa, E. B., LeBlanc, N. J., Bui, E., McSweeney, L. B., … & Rauch, S. A. (2017). Temporal sequencing of change in posttraumatic cognitions and PTSD symptom reduction during prolonged exposure therapy. Behavior therapy, 48(2), 156-165.
Meyer, E. C., La, H. B., DeBeer, B. B., Kimbrel, N. A., Gulliver, S. B., & Morissette, S. B. (2018). Psychological inflexibility predicts PTSD symptom severity in war veterans after accounting for established PTSD risk factors and personality. Psychological trauma: theory, research, practice and policy.
Mills, C. P., Hill, H. M., & Johnson, J. A. (2018). Mediated effects of coping on mental health outcomes of African American women exposed to physical and psychological abuse. Violence against women, 24(2), 186-206.
Ogle, C. M., Siegler, I. C., Beckham, J. C., & Rubin, D. C. (2017). Neuroticism increases PTSD symptom severity by amplifying the emotionality, rehearsal, and centrality of trauma memories. Journal of personality, 85(5), 702-715.
Oravecz, R., Penko, J., Suklan, J., & Krivec, J. (2018). Prevalence Of Post-Traumatic Stress Disorder, and Coping Strategies Among Slovene Medical Emergency Professionals. Sigurnost, 60(2).
Otis, C., Marchand, A., & Courtois, F. (2012). Risk factors for posttraumatic stress disorder in persons with spinal cord injury. Topics in spinal cord injury rehabilitation, 18(3), 253-263.
Reid, M. D. (2005). Memory as initial experiencing of the past. Philosophical Psychology, 18(6), 671-698.
Reisman, M. (2016). PTSD treatment for veterans: What’s working, what’s new, and what’s next. Pharmacy and Therapeutics, 41(10), 623.
Runyon, M. K., Deblinger, E., & Steer, R. A. (2014). PTSD symptom cluster profiles of youth who have experienced sexual or physical abuse. Child abuse & neglect, 38(1), 84-90.
Sauer, J., & Bhugra, D. (2001). Drug treatments in post-traumatic stress disorder. International Review of Psychiatry, 13(3), 189-193.
Seligowski, A. V., Miron, L. R., & Orcutt, H. K. (2015). Relations among self-compassion, PTSD symptoms, and psychological health in a trauma-exposed sample. Mindfulness, 6(5), 1033-1041.
Wisco, B. E., Marx, B. P., Holowka, D. W., Vasterling, J. J., Han, S. C., Chen, M. S., … & Keane, T. M. (2014). Traumatic brain injury, PTSD, and current suicidal ideation among Iraq and Afghanistan US veterans. Journal of Traumatic Stress, 27(2), 244-248.
Did you find any useful knowledge relating to Post-Traumatic Stress Disorder (PTSD) in this post? What are the key facts that grabbed your attention? Let us know in the comments. Thank you.
Cultural factors in diagnosis and treatment are highly imperative. This paper includes critical thinking on the perils of using mainstream methodology with non-Western cultures.
Cultural factors have deep roots in the clinical psychology. Cross cultural psychology has now become an inseparable idea in clinical psychology. Culture cannot be avoided in order to make a precise judgment on mental problem. The paper is based upon literature review on various academic articles and books written to cover the significance of culture in clinical psychology. It offers systematic review based upon authentic basis regarding psychological treatment considering the cultural factors involved in diagnosis. Efforts are expected to focus on accurate judgment, suitable therapeutic process and an eventual release of the painful feeling.
The capable psychoanalysts must be devoted, and eager to understand the cultural backdrop, past experiences and its correlation with the psychological diagnosis and handling of the case. Also a patient from non-western cultural background must be treated with extreme care while considering his cultural beliefs as important indicators to achieve optimum output; an ultimate relief for the patient.
Respecting the consensus developed by historic and contemporary professionals, a psychologist can enhance efficacy of the treatment and avoid the perils of the mainstream methodology in treatment of non-western cultures.
Cultural factors are one of the most significant variables in the field of clinical psychology. A clinician cannot aim for precise diagnosis and appropriate treatment without considering the culture of the patient as a guiding principle, as many of the psychological behaviours are directly influenced by the cultural norms.
The paper presents a review of different cultures and their requirement for the diagnosis of treatment on mental health problems. It will also highlight potential harms of applying mainstream methodologies on a non-western client. A detailed literature review will explain the main aspects of non-western culture and culture related attitude on mental health.
While treating the mental disorders, it will be useless if a general method is applied on everyone, without studying the socio cultural background of the client and salient features of the specific culture. We can explain its importance through an example; drinking habit may be a serious issue in a culture and may demand psychotherapy to get rid of it, but it is possible that it is considered as a normal thing in another culture.
Also shyness of a female towards the males can be considered as a psychological problem in the western culture, though it may be considered as a normal behaviour in non-western traditions. Any diagnosis cannot be appropriate unless it is seen through the lens of the culture. Every psychological disorder has a deep connection with religious beliefs, ethnic norms, and native environment.
An expert clinician has to identify that root first before making a professional judgment on the problem, type of treatment and therapeutic process required, and mannerism of the sessions, and required cultural sensitivity aspects during the therapies. The need of cognitive testing can only be identified after thorough analyses of the cultural factors behind the problem.
Cultural factors in psychological diagnosis and treatment; an overview
Psychological diagnosis is very much dependent on the symptoms in human behaviour. Talking about the general perception on mental illness or disorder, anything different from a usual behaviour is referred as a psychological disorder. These perceptions are closely related to the culture possessed by the patient and also the interpretation of any behaviour as according to the cultural norms.
We can understand this phenomenon by an example of some sort of mania. Mania is almost a common problem found in almost all the cultures, but the clinician must be very careful in diagnosis, as there is a probability of confusing the culture related expression of distress as wrong diagnosis of mania. We can observe cultural diversity in stating the depression, but it may be under diagnosed, usually on initial stage and careful measures are not taken.
It is true that somatic characteristics may be identical in all the cultures, yet, it is critical to differentiate physical descriptions of a sentimental situation. Generally ways of expressing depression are different in all the cultures, however, sad mood, unwillingness in enjoying something, nervousness, and feeling energy less are common symptoms of depression. Culture cannot be neglected for any sort of psychiatric treatment like, while classifying depressive disorders, for example, we have to consider both internal factors within the individual and external factors related to the culture of the subject (Cowen P. et al. 2012. p212).
In the discussion, as it follows, various culture factors will be elucidated as they influence psychological diagnosis and treatment in various situations. It is also important to know how the treatment can cause harm instead of healing the suffering if a client from non-western culture is dealt in mainstream methodologies of diagnosis and treatment.
Cultural diversities and mental health
Culture is an inherited asset which travels from generation to generation. This is a factor which has direct influence on all aspects of the lives of human beings. As far as the approach on mental problems is concerned, it varies from person to person, family to family; various ethnic groups, culture to culture and country to country.
It has been observed that culture and religion have a strong influence over the mental health of a person, and initiation of mental illness. Also cultural mannerism of responding towards such problems, determines the extent of agreement of the patient for mental sickness treatment and consistency in this regard. It is very important to understand that representation of mental wellbeing service demands cultural sensitivity for improving acceptance and awareness on the use of these services.
This will help to reform approach about mental illness, as it is different from the one customary in the west. We can review a case study to understand this difference. This comparative study was conducted by universities in India and America, to compare behaviours in India and USA. It was found that the students from India perceived depression as an outcome of the factors like, being unsuccessful in achieving goals, or else which can easily be controlled by them individually, and felt that only way to manage depression is to ensure social facilitation and religious practices. They suggest that understanding and treating depression must consider diverse point of views on mental illness for enhancing the efficacy of mental wellbeing plans (Nieuwsma, J.A.et al. (2011). p 539-568).
Relationship of psychology and culture has been discussed by many expert psychologists, according to Triandis H.C. quoted by Kitayama S. and Cohen D. (2010), history of psycho-cultural tendencies have shaped the contemporary approaches of cultural psychology, and the future of this field is also based upon the same.
He emphasizes on the close connection of the language; a salient feature of each culture, and psyche. He believed that language is the key to understand the thoughts of the speaker. Due to interaction of various people within the same culture, many agreements are found on the ways to behave collectively. These practices by the time shape the mind accordingly, thus we can say, an individual expresses his culture which he has been brought up (Kitayama S. and Cohen D. 2010).
Mental illness as a stigma in various cultures
Perceiving mental disorder as a shameful fact may be due to many reasons, for example, any of the apparent reason of the sickness. Many studies have reported other major distinctions in behaviour towards mental illness amongst cultural groups in the USA. Carpenter-Song et al. (2010) performed a thorough, one and a half year long culture based study.
The subjects for the study were 25 patients with critical mental illness. These were European-American patients engaged in regular treatment by expert psychiatrist, inclined to state convictions about mental sickness associated with medical viewpoints about the illness. Contrary to this, people belonging to Africa, America or Latin patients were more liable to highlight non-medicinal explanations about the signs of mental disorders.
Though, all the subjects from 3 cultural clusters shared about some sort of stigmatization because of their mental problems, this very shamefulness sentiment proved to be a main part of the African-Americans reactions, hence it was not focused in case of European-Americans, instead they inclined to consider mental problems as major and most important side of the human requirements on health.
As far as African-Americans were concerned, they were frustrated when the clinicians emphasized on the need of medication. In case of Latin persons, they generally considered diagnosis of mental sickness to be a severe damage to their social image and status; they focused on stating the sickness on a very low severity to stay safe from extreme stigma (Carpenter.S. E. (2010) p 224-251).
As argued earlier, when we talk about stigma, its severity may be different in different individual cultures, which refers to a diverse nature in western and non-western cultures. In the non-western culture, sentiment of dishonour linked with mental disorder is very high. In such cases a mental situation, in which the patient thinks as if he is humiliated or not cared by anyone, leads to extreme loss of self-belief; thus the symptoms of mental sickness may even enhance.
Another evaluation of the association between ethnicity & cultural beliefs and mental disorders is conducted by Abdullah et al. (2011). This study illustrates thoughts on broad diversity of culture related ideas embedded in mental condition. For instance, a number of the cultures may not regard mental disorder as a cause of disgrace, some of those only focus on the extreme problems but others may feel shame on disorders of any level of problem. Generally, non-western people are highly anxious about their traditions, self-control, individual associations and expressive connections, mental illness is taken as shameful dilemma, not only for the specific person, but for the whole immediate and extended family. (Abdullah et al. 2011)
Resistance from the patients
Bailey et al. (2011) have shred about reluctant behaviours regarding mental treatment. He notes that sense of being ashamed, religion related misconceptions, lack of trust on the clinicians and language barriers and communication issues may be the reason behind this resistance in opting for mental health treatment as required (Bailey, R.K.et al. 2011 p 548-557.) In certain cultures clients show a lot of resistance just to satisfy their self-respect that they are normal and it will be real dishonour if they admit and accept need for mental treatment.
That is the main reason behind the concept that understanding culture of the client is very important, so as to understand the root causes of the resistance and reluctance. During the therapies, the clinician must develop a good rapport with the client, which is only possible with some awareness on the culture of the client. An expert clinician must focus on building a good relationship with the client during a few initial therapeutic sessions.
It may be performed through friendly discussion demonstrating interest in getting awareness on the client’s culture, which must be complemented through attempts to gain knowledge on the same through books and other sources, such as, friends and family of the client, other members of the same community and other internet sources.
This way the client will share many thoughts from his subconscious, and the root may be identified, along with a great control over the expected resistance from the client. Especially when we talk about non-western culture; as argued earlier; their stigma may be a great source of resistance. This can be overcome, if the client receives friendly signals from the clinician, and a sense of trust worthiness for thought sharing.
Cultural sensitivity while treating non-western clients
Generally, Non-western clients, especially Muslims adhere to their religious beliefs; therefore, it is crucial to be aware on the cultural heritage, and religious background of the Muslims for the contemporary psychologists, so as to ensure efficacy of the treatment, as this group of clients is rather difficult and needs to be understood properly. We have a discussion about the Muslim cluster in the non-western culture as it the biggest majority group in the non-west representation.
Considering religion, as a central point of the human life, makes it possible for a practitioner to manage therapeutic process with a high level of skill and anticipation of the optimal output, when tackled in religious framework. Religious beliefs, spiritual thoughts and mental health have an interesting correlation to apply for treating several mental disorders efficiently. Keshavarzi H. and Haque A. (2014) in an article highlight the need of improving the psycho-treatment procedures with the help of its integration with the culture and religious values, while treating Muslims for psychological disorder.
Religious faiths about the reason of mental sickness are typically unconnected to biological systems. Most of these are considered as a curse due to any bad deed in the past, or due to some spirits. However these symptoms may be different in the young and old generations. Also the nature of sickness differs in the native non-western client and second generation borne in a different culture. (Keshavarzi H. and Haque A. 2014)
Keshavarzi H. and Haque A. (2013) also quote Veling et al., (2008) who have highlighted non-western tendency of community based culture. It is a general norm that Muslim are fond of replication of a community environment similar to the native culture, wherever they live, such as community centers, caring for right of neighbours, selfless attitudes, mutual reliance and family values. These strong bonding practices generally tend to reduce chances of mental problems.
Cultural Factors Psychology
Lack or absence of cultural knowledge, especially on religious faith, norms and practices by non-Muslim therapists may be a hurdle in creating a remedial association with the client. It is important to be aware of certain practices which are extremely conflicting with Muslim cultures as observed in the west. Male and female interaction can be one of the examples, which is extremely prohibited in Muslim culture, though considered a normal matter in other cultures. This can lead to a serious problem during the sessions, if not understood according to the cultural requirements. For the therapist, it is also recommendable to make collaboration with religious leaders, so as to enhance religious understanding on the Muslim psyche and Islamic modes of treatment (Keshavarzi H. and Haque A. 2013).
We see that there is lack of sufficient materials on culture specific treatment methodologies for non-western clients. Many therapeutic concepts cannot be applied on the non-western client the way these may probably be efficient for the western client. Treatment of non-western client, though complicated, it also holds many helpful resources within its roots.
As we see that in the non-western culture, family values and social relationships are highly cherished. These may a helpful tool for resource mobilization. To cope with language barriers family members can be a helpful resource. Another precaution is also recommended by Cowen P. et al (2012) that assigning a translator during sessions also demands special care about the selection of the person to interpret. As a general observation it is a fear that involving a translator, other than the therapist himself, may cause difficulty to achieve specific results, besides ever-increasing the duration of the meeting. Mare transformation of the language may not be helpful while the person is not a health expert, sometimes the spirit of the conversation is lost while translation process.
This problem can only be conquered with the help of same community members, close family relation, or assigning a professional psychologist, the responsibility to communicate and interpret with the non-western client, and then be a part of diagnosis and therapeutic process. These dissimilarities are not exclusive for Muslims only; the other representatives of the non-western culture, such as Hindus and Buddhist are also different in terms of their traditions, norms and their approach towards mental illness, from the western culture. The same requirement of studying the specific culture persists for the therapist for a patient who belongs to any of these cultures (Cowen P. et al 2012).
All these arguments on the study of clinical psychology elucidate that dealing mannerism must represent adaptability according to the requirement of the culture when handling patient from a culture, which the therapist does not belong to. It must be understood that mainstream psychological methodologies might not fulfill the extraordinary needs of the situation.
It is also quite natural that a single person may not possess the knowledge about each and every culture in the world, which makes things more complicated for the psychologist to have the anticipated outcomes. In some cases patients may even assume biased behaviour from any person or a group, financial stress, and a feel of inaccessibility to services if he is uncomfortable in any other culture, this might transform into the symptoms of mental illness later on. As a general observation, most of the cases of migrants emerge due to adaptability issues and may become severe if not handled on time with due diligence (Cowen P. et al 2012. p. 26. Ch 3).
As argued earlier, mental health issues with the systematic application of connection with the clients may notably increase because, most of the issues come forward because of cultural intricacy. Even the best knowledgeable practitioner may not be able to ascertain mental well being of a patient, if, he does not make himself well aware of the culture; the patient is coming from, and all probable cultural approaches which may be contributing in increase of mental illness motives in the subconscious of the patient.
The contemporary studies emphasize that culture has unambiguous connection with psychological problems. A psychotherapist must not stress on conservative systems of treatment, and bring in inventive thoughts in accordance to the requirement and judge diverse features of cultural psychology (Tseng W.S 2008).
As we learned from Keshavarzi H. and Haque A. (2014), that initial effort for applying the psychological approach is the precise judgment of the issue and the performance level of the patient. In this regard, the therapist has to collect information which is essentially required for treatment. If the judgment indicates a high tendency of the client towards religion, the therapist must take that into account. This may be evaluated during initial informal discussions through the use of terminologies and his general approach.
The clinician must have an intention to develop an understanding with the patient on how the objective of the treatment is set. Later, a detailed session should be conducted to assess how he expects the improvement as a result of the therapeutic process. If the patient does not take interest in self-actualization, and wants focused attention to the specific problem, therapist must not resist, and make the client comfortable, removing discomforts of cultural difference (Keshavarzi H. and Haque A. 2014).
When we talk about the cultural beliefs in Arabian culture we cannot exclude religious and traditional methods of the psychotherapies. The majority of the Arabs rely on conventional healers, also referred as faith healers, such as experts of herbal medicines, religious elders of the region, healing through rituals. Unfortunately the initial level of mental disorder is assumed to be an assault of evil spirits such possession of the body, which can just be treated with the help of rituals. Treating the mentally ill person is believed as a punishment for the patient, that might mark him as a crazy or abnormal person forever, thus restricting hi normal movement in the in the society for the rest of his life (Parekh R. 2013).
The most complex idea about this subject is the command of a clinician about the features of every culture. Though it is not simple but the clinician must be open to learn about the cultural features which truly have an effect on the healing procedure. Cultural knowledge compliments the success of the healing procedure by demonstrating respect for the patient and the culture. The most important aspect of the point is that a proficient psychologist must be impartial, enthusiastic, and considerate on the cultural surroundings, the history and its link with the course of analysis and therapy.
The whole discussion stressed over an idea that culture and psychology cannot be viewed in isolation; we cannot suppose on the performance of brain and a culture bound psychosomatic approach, linked with one culture and expected to apply in any other culture, these aspects must be taken into account during therapeutic process.
While treating non-western clients, we must be clear on a few general distinctions in the culture, Such as:
Adaptability issues
Effect of religious beliefs on psychological beliefs
Strong family bonding
Reluctance of women on open communication with a male therapist,
Entirely different social environment
Less preference of psychological treatment as compared to physical issues.
Language barrier
Keeping all these aspects in mind, a clinician has to show respect for that cultural characteristic to develop outstanding professional relationship with the patients. Talking about sentimental problems in a responsive manner may help in this regard, because, general tendency of the non-western clients demonstrates shyness in discussing personal events, which may point towards the roots of the problem which may be linked with the cultural beliefs. Thus, to discover secrets of the subconscious, information on the patient’s culture is unavoidable.
As we have already discussed that family bonding and social relationships are very strong in the non-western culture, these may also give rise to some problems related to the expectations associated with these values. These false expectations may give birth to a feeling of disappointment or betrayal from a close person. It also makes them feel that those people have wasted their sacrifices and have not cherished their support. This leads to anger and fury for their own selves as well as for others.
This also gives rise to hopelessness, and trust over others including their psychologist. It can also result into discontinuation of constructive attitude; which generates dire need of family support, counselling and cognitive therapy with individual. A feel of being deprived regarding marital rights can be an example of such cases. These sort of cases are culturally sensitive and may be dealt with high care, after acquiring sufficient knowledge of the specific cultural values and norms (Keshavarzi H. and Haque A. 2014).
Mainstream methodologies: Benefits and Perils
Before concluding the paper, we must focus on the perils of the mainstream methodologies when applied in non-western culture. During our argument, one thing has been concluded that we cannot study psychotherapeutic treatment in isolation; culture must be included in the analytical process. We can classify the type of clients in two culture specific groups:
Western culture
Non-western culture
Both have very clear dividing lines for general understanding on cultural beliefs. As we conclude that cultural beliefs play a major role in psychiatric diagnosis and treatment. The very first step involves the basic understanding on the culture of the patient and to what extent these beliefs and norm influence his cognitive behaviour. Though these are the two basic cultural groups, the non-western cluster may further be divided into more clusters based on religion and geographic trends.
Muslims; the largest group in the non-western culture are more influenced by the religious education, rituals, spiritual treatment and other limitations. The beliefs of the patients may not be agreed by the practitioner, however it is important, not to argue with the patient, and give him a feel that the practitioner believes him and respects his point of view. Other clusters within the non-western cultures should also be dealt accordingly. Suspicion on the clinician, being afraid of the treatment, being afraid of racist of discriminatory approach, language and communication barriers, and cultural & religious issues may hinder the successful treatment (Keshavarzi H. and Haque A. 2013).
This reaches the following understandings:
Considering culture is the most important aspect in psychological treatment.
Initial meetings should be focused on gaining awareness about cultural and religious tendencies of the patient.
Physical interaction between male and female is strictly prohibited in non-western culture; this must be avoided at any condition.
General methodologies may not be applicable to all the patients. In the study of psychology, every client has his unique identity, he must be dealt individually. The approach that proved to be successful for treating depression of a western women, may not work for exact replication for a non-western woman.
The clinician must not try to influence patient’s cultural beliefs.
The clinician must show respect for the culture to develop mutual trust and good professional relationship.
Mare translation is not enough for the sessions, the interpreter must be a professional therapist, or a family or community member of the patient if the first option is not possible.
Consultation with the family is also recommended when possible. This may also help to overcome stigma and seek early healing of the problem rather that making it worse due to delayed treatment.
Depressive disorders may be similar in different cultures, however, the therapist must study, what is hidden behind the symptoms, inside the cultural context.
Conclusion
As a concluding note we can easily claim that psychiatric diagnosis cannot be made leaving the cultural factors behind. Making an attempt to do so may lead to commit wrong diagnosis and ultimately a wrong treatment. In advanced clinical psychology, wrong diagnosis and treatment is as dangerous as an unnecessary medicinal injection.
A clinician has to demonstrate high level of professionalism and skill to handle the case with careful cultural sensitivity. There may be chances to disagree with the client belief, and also his cultural belief may be opposite from the therapist’s cultural norms, yet, he must not mention so in front of the client. There is high probability for resistance from the client and he also may show distrust on the treatment, however, the therapist has to be unbiased and temperamental. He has to make the client feel that his opinion is respected; being a leader or teacher may not be an appropriate approach, rather than being a facilitator.
As any unnecessary medicine may cause harm, in the same way, wrong approach towards cultural psychology may be equally harmful. A uniform methodology may not be applicable in all cases. If the client is under strong influence of religion and other features of the culture, it may not be ignored. A good rapport with the client is a half way towards the successful psychological treatment, and understanding the Cultural Factors is the map to reach this destination. .
References
Abdullah, T., Brown, T.L. (2011). Cultural Factors, Mental illness stigma and ethno-cultural beliefs, values, and norms: an integrative review. Clinical Psychology Review, 31: 934-948.
Bailey, R.K., Milapkumar, P., Barker, N.C., Ali, S., Jabeen, S. (2011). Cultural Factors and Major depressive disorder in the African American population. J Natl Med Assoc.,103: 548-557.
Carpenter-Song, E., Chu, E., Drake, R.E., Ritsema, M., Smith, B., Alverson, H. (2010). Ethno-cultural variations in the experience and meaning of mental illness and treatment: implications for access and utilization. Cultural Factors Transcultural Psychiatry, 47(2): 224-251.
Cowen P. Harrison P. Burns T. (2012). p.621. Ch 21. Shorter Oxford Textbook of Psychiatry Cultural Factors. Oxford University Press.
Keshavarzi H. Haque A. (2014) Integrating indigenous healing methods in therapy: Muslim beliefs and pract ices, International Journal of Cultural Factors and Mental Health, 7:3, 297-314.
Keshavarzi H. Haque A. (2013) The International Journal for the Psychology of Religion and Cultural Factors, 23:230–249.
Kitayama S. and Cohen D. (2010). Handbook of Cultural Factors psychology. Guilford Press.
Nieuwsma, J.A., Pepper, C.M., Maack, D.J., Birgenheir, D.G. (2011). Cultural Factors perspectives on depression in rural regions of India and the United States. Transcultural Psychiatry, 48(5): 539-568.
Parekh R. (2013) The Massachusetts General Hospital Textbook on Diversity and Cultural Factors in Mental Health Springer shop
Tseng W.S (2008). Cultural Factors and Psychotherapy: Review and Practical Guidelines Sage Publications.
WonPat-Borja, A.J., Yang, L.H., Link, B.G., Phelan, J.C. (2012). Cultural Factors Eugenics, genetics, and mental illness stigma in Chinese Americans. Soc Psychiatry Psychiatr Epidemiol., 47(1): 145-156.
According to DSM-IV-TR (the Diagnostic and Statistical Manual of Mental Disorders, fourth edition, text revision) personality disorders are defined by maladaptive personality characteristics which begin during early years of life and have serious and consistent effects on functioning (Diagnostic and statistical manual of mental disorders, 2000). Borderline personality disorder (BPD) is a common reason to visit a psychiatrist (Skodol, Gunderson, Pfohl, Widiger, Livesley & Siever, 2002). BPD affects 2 percent of adults (mostly young women) (Swartz, Blazer, George & Winfield, 1990). Patients with BPD present a high rate of self-injury (without intent of suicide) and a significant rate of suicide attempts and completed suicide (Soloff, Lis, Kelly, Cornelius & Ulrich, 1994).
The patients of BPD are many times in need of mental health services and approximately 20 percent of hospitalizations in the psychiatric department are of BPD patients (Zanarini, Frankenburg, Khera &. Bleichmar, 2001). A patient with depression or bipolar disorder mostly endures the same mood for weeks while a patient with BPD may experience angers (intense bouts), anxiety and depression that may endure for only hours or at the most for a day (Zanarini, Frankenburg, DeLuca, Hennen, Khera & Gunderson, 1998). A study performed by Zanarini & Frankenburg (1997) showed that most of the patients with BPD report a history of neglect, separation (as young children) or abuse. Another study performed by Zanarini (2000) concluded that 40 % to 71% of Borderline Personality Disorder & Attachment Theory.
Origin of Borderline Personality Disorder
Children who have been exposed to psychological and physical neglect, sexual and physical abuse and maltreatment are at risk of developing BPD. The mental trauma faced by these children is due to neglect and abuse by a primary caregiver. This trauma disrupts the normal and healthy development of secure attachment. And as a result these children develop disorganized attachment (anxiety and depression). The children who are neglected are at risk of social rejection, incompetence feeling and social withdrawal. Neurobiological dysfunction can be caused because of abuse and neglect by primary caregiver. In order to develop a capacity of regulating emotions and developing a coherent sense of self the child has a requirement of attachment from the primary caregiver.
Attachment Theory and Borderline Personality Disorder
As per the ethological perspective of John Bowlby (1977, 1980, 1991) BPD can be considered as a condition of significant insecure attachment (with significant oscillations between detachment and attachment & between yearning and longing). The working models present in affect regulation and a lack of coherence (mainly in relationships with others) (Bowlby, 1973). The sorrow of detachment faced in early childhood negatively impacts the psychology of the person and this result in heightened sensitivity to loss and separation. It is also important to note here that since these feelings and thoughts are disconnected to the happenings in early childhood these individuals are unable to understand the reason behind their reaction. Research scholars (Melges & Swartz, 1989) have compared the fluctuations in the behaviour of BPD patients to prickly porcupines – they are of the opinion that patients with BPD are in need of someone but when someone comes close to them they drive themselves away as a result of fear. Thus BPD patients are looking for secure attachment but they fear rejection, anxiety and anger that could result (Bowlby, 1979). Melges and Swartz (1989) are also of the opinion that patients with BPD are preoccupied with regulating space. They do not feel the “invisible elastic” of attachment (Bowlby, 1969, p. 45). Also they are unable to protect themselves from anxiety of separation (Adler & Buie, 1979). The influence of certain types of experiences as related to family can be the cause of separation anxiety (Bowlby, 1988). John Bowlby’s “The seminal developmental theory” for treatment of BPD patients (Bowlby, 1969; Bowlby, 1973; Bowlby, 1980) has gained great attention. Bowlby proposed that human beings face pressures of natural selection in order to evolve behavioural patterns (example, clinging, smiling and proximity seeking ), that evoke in adults the caretaking behaviour (example, soothing, holding and touching).
These behaviours are reciprocal and encourage the development of an affective and enduring tie between caregiver and infant, which forms attachment. It is the result of these parental responses that internal models of the self and others are developed in infants which act as templates in the functioning of relationships later in life (Bowlby, 1973).
The Findings and Proposals of Bowlby the Following Is True In Case Of Attachment (Bowlby, 1973)
1. Model Of Self: The Internal Working Of It Is Related To The Degree Of Acceptance And Love One Has In The Eyes Of Primary Attachment Figures.
2. Model Of Others: The Internal Working Of It Is Related To How Available And Responsive Attachment Figures Are Expected To Be.
Attachment plays a very crucial role in the development of an external environment from which the child develops a safe and secure internal model of the self. Security on the grounds of attachment as perceived by the child results in his or her exploration of the world with confidence; this confidence springs by the availability of the caregiver. Security in attachment thus promises consistent, coherent and positive self-image. It also provides a feeling of being worthy of love and expectation that the important ones to him or her will be responsive and accepting. We here note that Bowlby has presented to the scientific mind the importance and need of attachment as essential to infants and children. Thus, attachment can be considered as an essential ingredient in the production of a psychologically healthy life. Now let us consider BPD patients, it is a case where the security in attachment is absent and there is a split and malevolent representation of self and others (Kernberg, 1967). In the life of BPD patients we usually observe angry, manipulative and needy relationships (Benjamin, 1993).
A number of scientific studies and intellectual thoughts have considered that intolerance of aloneness is the main defining characteristic of BPD and it is essential to note here that the descriptive criteria of DSM are also of the same opinion (Adler & Buie, 1979). Thus, the concepts and theories of attachment in many ways relate to DSM diagnostic criteria. Gunderson (1996) proposed that the early attachment failures actually constitute the cause of intolerance. He noted that in times of distress and sorrow patients with BPD are unable to invoke a “soothing interject” and this is due to unstable and inconsistent attachments to early caregivers. The above proposed scientific thoughts of Gunderson (1996) are same as that of Bowlby’s concept of insecure attachment.
The Scientific Observations Of Gunderson (1996) The Following Points Are True In Case Of Patients With Borderline Personality Disorder:
A Feeling of Insecurity on Grounds Of Attachment, Especially Pertinent To:
Plea for Attention
Pleas for Help
Checking For Proximity
Clinging
A Feeling of the Following in Borderline Personality Disorder Patients:
Denial Of
Dependency Needs
Fearfulness About
Based on the comparison of theories of object relations and attachment (Lyons-Ruth & Jacobvitz 1999) distinguished between normal processes (in early development) of separation individualization from the disorganized conflict behaviour (for attachment figures) by toddlers who are at significant risk for development of psychopathology. She identified that in infants the disorganized insecure attachment as a risk factor in the later development of BPD. Thus, we can state that as per the findings of Lycos-Ruth those infants who are victims of insecure attachments during the early years of life are at risk of developing BPD during later years of their life.
Borderline Personality Disorder
Attachment Therapy
In 1990, ATTACh (Association for Treatment and Training in the Attachment of children) was created in order to address the need of society and families to deal with critical attachment and bonding issues. ATTACh has cited important principles of attachment therapy and this includes the following:
1. Attachment therapy can be defined as a therapeutic process that is designed with the aim to define, develop and promote reciprocal attachment relationship and that which completely meets the criteria of that therapeutic process as defined and developed by ATTACh.
2. The aim of treatment by attachment therapy is to address the attachment problems and enable patients with healthy attachment relationships.
3. The emphasis in attachment therapy is laid on touch, physical and emotional closeness, reciprocal behaviours, empathy, atonement, communication, playfulness and humour. The attachment and bonding therapists are therefore required to treat with attention to the physical and psychological safety and wellbeing of the children and adults.
4. Family systems approach is of prime importance in attachment therapy. Thus there is need to correct child’s relationship with his or her primary caregiver.
5. It is essential to assess and study the following;
Psychological history
Educational history
Treatment history
Medical history
Attachment & Social history (including breaks in attachment)
Developmental history (including prenatal and birth)
Intellectual and Cognitive skills and deficits
Family functioning
Differential diagnosis (including DSM and ICD diagnoses)
6. Parents and children form the most active group of treatment regimen. Attempts are made to develop healthier patterns of interaction and communication.
7. To assist parents to develop parenting strategies in order to support positive attachments.
8. Description of any shortcomings attachment therapy might have for treating this issue and what else could be fused with attachment therapy to meet these needs.
Criticisms of Attachment Therapy
1) The application of attachment therapy for treatment of patients with BPD is equated with rebirthing or holding therapy and the techniques used to achieve the results are dangerous.
2) During the treatment of patients with BPD the attachment therapists make use of criteria that are even beyond those provided by the DSM-IV-TR (Zeanah 1996; Boris et al 2004). The strong correlation between insecure attachment and pathological parent-child interaction as shown by attachment therapy are beyond the symptoms listed in the DSM criteria (Bowlby 1944, 1973).
3) The attachment therapists many times over diagnose BPD.
Almost 87% to 96% of the children, who experience abuse, neglect or both, show an insecure attachment (Crittenden, 1988).
Between 50% and 80% of the adopted children have attachment disorder symptoms (Carlson, Cicchetti, Barnett & Braunwald, 1989).
Approximately 20% of children living in homeless shelter and nearly two thirds in foster care are identified with attachment disorders (Boris, Wheeler, Heller & Zeanah, 2000).
4) Attachment therapy is not supported with “empirical evidence” While attachment therapy can provide treatment of BPD, studies have revealed the effectiveness of other therapeutic methods as well. These methods have been briefly described below:
1. Psychotherapy
Randomized controlled studies have presented the efficacy of dialectical behaviour therapy and psychodynamic / psychoanalytic therapy (Bateman & Fonagy, 2001). The treatment provided in these trials comprises of three key features;
Meetings with an individual therapist (once a week)
Group sessions (one or more in a week)
Meetings of therapists for supervision or consultation
The psychotherapist’s approaches include a building of a strong therapeutic alliance and monitoring the suicidal or self-destructive behaviours. Other essential component of effective treatment plan for patients with BPD includes managing feelings, promoting reflection action (and not impulsive action), reducing patient’s splitting tendency, and limiting the behaviours related to self-destruction. There is some empirical data that supports individual psychodynamic psychotherapy.
2. Group Therapy
Group therapy for BPD patients is supported with research findings that indicate that it can be helpful (Greene & Cole 1991). Note: However, the benefit of family therapy in the treatment of BPD patients is not evaluated yet with research studies.
Descriptions of how dimensions of cultural context impact the issue you are discussing. How might this inform your treatment? I strongly believe that psychologists should not be racists. Today we are required to treat patients of different ethnic groups and countries during our clinical practice. Even an expression of detachment or neglect can hurt hard the patients with BPD. As discussed above the patients with BPD are in need of love and acceptance, care and attachment, understanding and touch, soothing approach and closeness. If a psychologist will distinguish on the grounds of colour, race, region and country then s/he won’t be able to perform well because for the treatment of BPD patients with attachment therapy it is essential to shower true attachment. Roentsch (1985) defines racism as: “Let there be no misunderstanding. A racist is anyone who accepts the existence of racial collectives”. Amongst doctors there is a belief in the a priori inferiority of non-white (Eysenck, 1990: pp. 215-220). The facts on racism reveal that we divide the world into ‘in-group and out-group’ or ‘us and them’ (Baron and Byrne, 1994: pp. 228-229). An important study first conducted by Clark and Clark (1947, in Baron and Byrne, 1994: 256) showed that a significant proportion of non-white children had internalized the attitudes of white racist. Thus the reaction of non-white adolescents towards white psychologists can be considered to be different from the reaction towards non-white psychologists. These racists’ feelings need to be addressed with maturity and patience. The dealings, behaviour and communication need to be such monitored that the feeling of racism is absent.
Self-issues that may impact a clinician’s conceptualization and treatment of this issue from an attachment perspective. How might one’s cultural context inform what they see and how they see it? What should clinicians be cautious of? Bonus points for examination of your own “self” in relation to treating this issue from an attachment perspective.
During my school times I lost my best friend because of racial differentiation attitude of a teacher. I was very much in harmony with my non-white friend. We had a high level of understanding and we loved spending time together. We were best friends for 3 years. However, my teacher did not like us being friends. She was white and disliked non-white people. Though she did not show it openly but it was obvious by some of her remarks at different times about non-white people. My teacher asked me to quit my friendship with the non-white girl. At first I was very much hurt by my teacher’s approach but then I agreed to it. This is because my teacher said that she will assure that I will get better grades in school if I agreed to what she said. My friend was very much hurt when I broke friendship with her. And after doing this I felt guilty for doing something really wrong. Even several years after quitting friendship with her, I feel sorry for my decision. Actually for some part of my life I had started thinking the way my teacher thought. I use to respect my teachers and had a feeling that they are always right. This is the reason why I started feeling that my teacher’s attitude towards non-white people was right. However, my thoughts have changed to good after leaving school. Now, I am equally friendly towards both non-white and white. I have both non-white and white as my friends. But sometimes the thought that I was once a racist makes me feel guilty. When I recollect that I was once a racist, I lose confidence in dealing with non-white people. I noted this when I was working on the treatment of a BPD patient who was non-white. I need to be more confident in my dealing with non-white people. I need to feel sure that I no more differentiate between non-white and white. I think I will gain this confidence when as a result of my sincere work several non-white BPD patients will get healed.
Describe what the early, middle and ending phases of therapy might look like for treating this issue based on what you have learned. Please also include some possible interventions and assessment methods. Attachment theory has been applied to both children and adults suffering from detachment. Bowlby (1969) formed a lifelong attachment behavioural system which encourages secure attachment. The attachment thus begins with the child’s requirement of secure attachment from the primary caregiver. The behaviour of attachment is organized and revolves around primary care giver. The feelings of attachment are elicited during the period of mental or physical discomfort or stress (1969). As per Bowlby’s (1969) perspective BPD can be considered as a condition of significant insecure attachment. There exists number of oscillations between detachment and attachment. The early childhood experiences of BPD patients are that of detachment, neglect, abuse, separation and loneliness. Thus the systems that mediate the feelings of attachment and positive behaviour are distorted and deactivated. In addition to this BPD patients have intense fear linked with loss and separation. However, since BPD patients do not remember their childhood time when they were neglected and abused they are unable to understand the reason behind their behaviour. I think a therapist is required to develop a secure and genuine attachment relationship with the BPD patients. The patient should feel completely secure in his or her relationship with the therapist. S/he should have no fear of loss or separation as related to relationship with the therapist. Development of a ‘secure’ attachment can help establish happiness in the life of the patient.
BPD patients are in need of love but the fear of loss and separation drives them away from people. It is therefore crucial that this fear of loss and separation should be dealt in the first phase of treatment. The patient with BPD should be counselled in such a manner that s/he starts gaining confidence in building secure relationships. The approach of the therapist should be driven by ‘attachment’ and ‘love’. Thus, while attempting to heal the BPD patient of the fear of separation, the therapist should try to build his or her own place in the heart of the patient. The approach should not only aim to heal the fear but also to open ways for love and attachment. The therapist should make the patient feel that s/he really cares for him. That it is not just a routine responsibility or duty to address the need of the patient. The therapist should show that s/he has started loving the patient and has become attached with him. S/he has started caring for the needs and essential requirements of the patient. A feeling of attachment should spring from within the heart of the therapist and should touch the emotions of the patient. Parents of the patient should be educated on the basics of attachment.
They should be taught the need of touch, eye contact, motion, love, compassion, care and attachment. The issues related to behaviour should be addressed and the pitfalls should be examined. The treatment should include a review of the attachment issues of the parents’. The parents should be educated on good ways to bring up the child. The attachment from parents and primary care taker are essential for answering the need of BPD patients. Gregory C. Keck states that holding the child or adolescent gives rise in an emotional response and intensity that cannot be achieved by any other medicine or therapeutic regimen. Therapist should educate the parents or the primary caretaker to hold the child or adolescent. The therapist should work to build in attachment between the child/adolescent and the parents/primary caretaker. Building of relationship and providing security and affection from parents or primary caretaker should be assured.
The therapist should also spend time to build in attachment between the child/adolescent and himself
The therapist should also work to repair the relationship that has been broken. S/he should try to develop more peaceful and lovable feelings between the child/adolescent and the parents/primary caretaker. The therapist can also do the holding of the child/adolescent and then s/he can transfer the responsibility to the parent or primary caretaker. The therapist is also required to make an important clinical judgment with regard to the suitability of the primary caretaker or parent for such an attachment. Guidance and education as related to the attachment should be provided by the therapist. In addition to holding ‘eye contact’ is an important part of attachment therapy. Eye contact opens the door to the heart of the person and builds attachment.
In conclusion, the therapist should believe in building relationships of attachment. A feeling of security should be the base of such attachments. Broken attachments should be repaired and new attachments should be built-in. The therapist should form attachment of the patient with himself or herself. In addition to this attachment should be built between the parent/primary caretaker and the child or adolescent. Education should be imparted on developing attachment. Today, in the modern days parents find little time for their children. Many times they forget to care for their own child. The child gets hurt each moment by a lot of anxiety, depression, neglect and loneliness. The child loses the charm of attachment and feels that s/he won’t get attachment from anyone. I believe that in order to begin with attachment therapy it is essential for the therapist to first build attachment between himself and the child/adolescent. Therapist should also build in attachment between himself and the parents of the child/adolescent. This is because the parents who feel attachment from the therapist will be more responsive and agreeable to treatment.
Attachment Can Create Wonders in the World of Therapy and Therapeutics
Attachment speaks to the heart and touches the emotions to bring forth a feeling of recovery. I strongly believe that attachment therapy is the best suit for patients with BPD. This is because attachment can repair the broken hearts, the fading hopes, the dying relationships and the detached home. I would strongly recommend attachment therapy as a method of choice for the treatment of patients with BPD. Children and adolescents want someone to speak to their heart, someone who understands their need of attachment and addresses to their requirement of love, touch, care and affection. During all the phases of treatment this should be kept in mind and should be reflected in approach and practice of the therapist.
Conclusion
Attachment theory is a good addition to the knowledge of psychology and its application can be beneficial for the treatment of BPD patients. While dealing with patients of BPD the psychologist should not have racist attitude and his or her approach should be confident.
References
Adler, G., Buie, D. H. Jr. (1979). Aloneness and borderline psychopathology. The possible relevance of child developmental issues. Int J Psychoanal, 60, 83–96
Baron, R. & Byrne, D. (1994). Social Psychology (7th ed.,). MA: Allyn and Bacon, Boston
Bateman, A. & Fonagy, P. (2001). Treatment of borderline personality disorder with psychoanalytically oriented partial hospitalization: an 18-month follow-up. Am J Psychiatry, 158, 36–42
Benjamin, L. S. (1993). Interpersonal diagnosis and treatment of personality disorders. New York: Guilford
Boris, N. W., Hinshaw-Fuselier, S. S., Smyke, A. T., Scheeringa, M. S., Heller, S. S. & Zeanah,
C. H. (2004). Comparing criteria for attachment disorders: establishing reliability and validity in high-risk samples. J Am Acad Child Adolesc Psychiatry, 43(5), 568-77
Boris, N. W., Wheeler, E. E., Heller, S. S. & Zeanah, C. H. (2000). Attachment and developmental psychopathology. Psychiatry, 63, 75-84
Bowlby, J. (1944). Forty-four juvenile thieves: Their characters and home life. International
Journal of Psychoanalysis, 25, 19–53
Bowlby J. (1969). Attachment and loss. Vol. I: Attachment. New York: Basic Books
Bowlby, J. (1973). Attachment and Loss. Vol. 2: Separation, Anxiety, and Anger. New York: Basic Books
Bowlby, J. (1979). Psychoanalysis as art and science. International Review of Psycho-analysis, 6(3), 3-14
Bowlby J. (1980). Attachment and Loss. Vol. 3: Sadness and depression. New York: Basic Books
Bowlby, J. (1991). Charles Darwin. New York: W. W. Norton
Carlson, V., Cicchetti, D., Barnett, D. & Braunwald, K. (1989). Finding order in disorganization: Lessons from research in maltreated infants’ attachments to their caregivers
Cicchetti & V. Carlson (Eds.), Child Maltreatment: Theory and research on the causes and consequences of child abuse and neglect. New York: Cambridge University Press
Crittenden, P. M. (1988). Relationships at risk. In J. Belsky & T. Nezworski (Eds.), The clinical implications of attachment (pp. 136-174). Hillsdale, N.J.: Lawrence Erlbaum
Diagnostic and statistical manual of mental disorders. (2000). (4th ed.) [text revision] Washington: American Psychiatric Association.
Eysenck, H. J. (1990). Rebel With A Cause. London: W H Allen and Co.
Greene, L. R., Cole, M. B. (1991). Level and form of psychopathology and the structure of group therapy. Int J Group Psychother, 41, 499–521
Gunderson, J. G. (1996). The borderline patient’s intolerance of aloneness: insecure attachments and therapist availability. Am J Psychiatry, 153, 752–8
Kernberg, O. (1967). Borderline personality organization. J Am Psychoanal Assoc, 15, 641–85
Lyons-Ruth, K. & Jacobvitz, D. (1999). Attachment disorganization: unresolved loss, rational violence, and lapses in behavioral and attentional strategies. In J. Cassidy & P. Shaver (Eds.), Handbook of attachment: theory, research, and clinical implications (pp. 520–44). New York: Guilford.
Melges, F. T. & Swartz, M. S. (1989). Oscillations of attachment in borderline personality disorder. American Journal of Psychiatry, 146(9), 1115-1120
Roentsch, D. (1985). Racists define Racism. In The Radical Capitalist (USA), 3(4), 2-6
Skodol, A. E., Gunderson, J. G., Pfohl, B., Widiger, T. A., Livesley, W. J. & Siever, L. J. (2002). The borderline diagnosis. I: Psychopathology, comorbidity, and personality structure. Biol Psychiatry, 51, 936-50
Soloff, P. H., Lis, J. A., Kelly, T., Cornelius, J. & Ulrich, R. (1994). Self-mutilation and suicidal behavior in borderline personality disorder. Journal of Personality Disorders, 8(4), 257-67
Swartz, M., Blazer, D., George, L. & Winfield, I. (1990). Estimating the prevalence of borderline personality disorder in the community. Journal of Personality Disorders, 4(3), 257-72
Zanarini, M. C. (2000). Childhood experiences associated with the development of borderline personality disorder. Psychiatric Clinics of North America, 23(1), 89-101
Zanarini, M. C. & Frankenburg, F. R. (1997). Pathways to the development of borderline personality disorder. Journal of Personality Disorders, 11(1), 93-104
Zanarini, M. C., Frankenburg, F. R., DeLuca, C. J., Hennen, J., Khera, G. S. & Gunderson, J.
G. (1998). The pain of being borderline: dysphoric states specific to borderline personality disorder. Harvard Review of Psychiatry, 6(4), 201-7
Zanarini, M. C., Frankenburg, F. R., Khera, G. S., &. Bleichmar, J. (2001). Treatment histories of borderline inpatients. Comprehensive Psychiatry, 42, 144-150
Zeanah, C. H., Scheeringa, M., Boris, N. W., Heller, S. S., Smyke, A. T., & Trapani, J. (2004) Reactive attachment disorder in maltreated toddlers. Child Abuse & Neglect, 28, 877-888